What seems like a usual day to a seasoned hospitalist can be a daunting task for a new hospitalist. A routine day as a hospitalist begins with prerounding, organizing, familiarizing, and gathering data on the list of patients, and most importantly prioritizing the tasks for the day. I have experienced both traditional and unit-based rounding models, and the geographic (unit-based) rounding model stands out for me.

Dr. Isha Puri
The push for geographic rounding comes from the need to achieve excellence in patient care, coordination with nursing staff, higher HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores, better provider satisfaction, and efficiency in work flow and in documentation. The goal is typically to use this well-established tool to provide quality care to acutely ill patients admitted to the hospital, creating an environment of improved communication with the staff. It’s a “patient-centered care” model – if the patient wants to see a physician, it’s quicker to get to the patient and provides more visibility for the physician. These encounters result in improved patient-provider relationships, which in turn influences HCAHPS scores. Proximity encourages empathy, better work flow, and productivity.
The American health care system is intense and complex, and effective hospital medicine groups (HMGs) strive to provide quality care. Performance of an effective HMG is often scored on a “balanced score card.” The “balanced score” evaluates performance on domains such as clinical quality and safety, financial stability, HCAHPS, and operational effectiveness (length of stay and readmission rates). In my experience, effective unit-based rounding positively influences all the measures of the balanced score card.
Multidisciplinary roundings (MDRs) provide a platform where “the team” meets every morning to discuss the daily plan of care, everyone gets on the same page, and unit-based assignments facilitate hospitalist participation in MDRs. MDRs typically are a collaborative effort between care team members, such as a case manager, nurse, and hospitalist, physical therapist, and pharmacist. Each team member provides a precise input. Team members feel accountable and are better prepared for the day. It’s easier to develop a rapport with your patient when the same organized, comprehensive plan of care gets communicated to the patient.
It is important that each team member is prepared prior to the rounds. The total time for the rounds is often tightly controlled, as a fundamental concern is that MDRs can take up too much time. Use of a checklist or whiteboard during the unit-based rounds can improve efficiency. Midday MDRs are another gem in patient care, where the team proactively addresses early barriers in patient care and discharge plans for the next day.
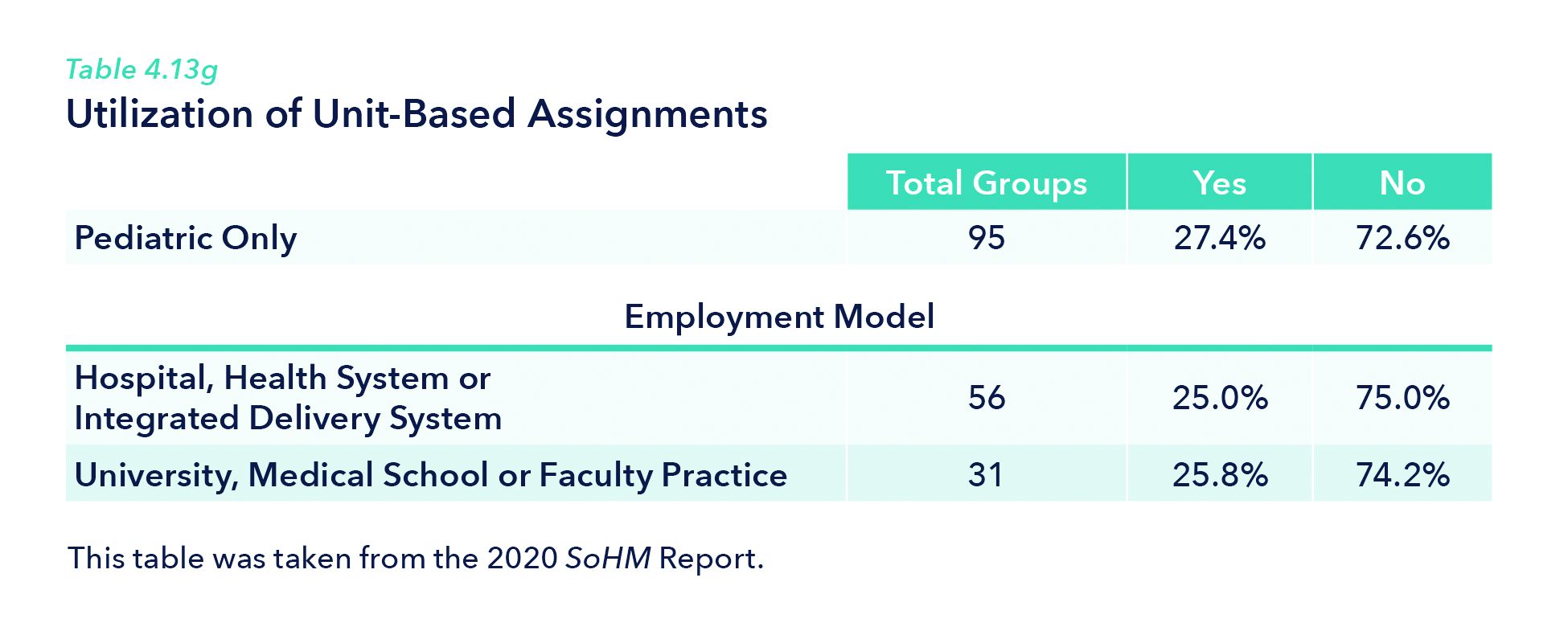
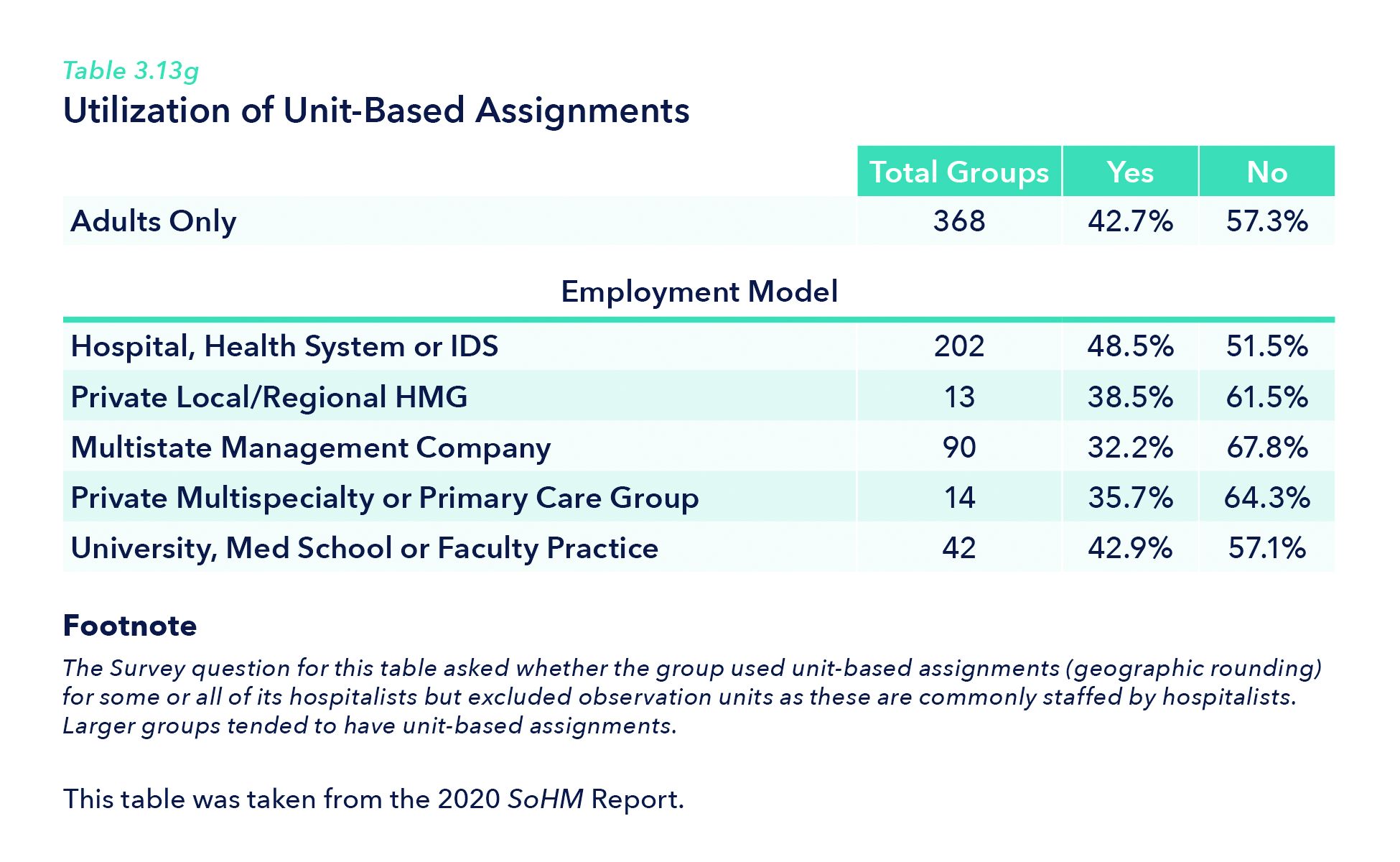
The 2020 State of Hospital Medicine report highlights utilization of unit-based rounding, including breakdowns based on employment model. In groups serving adults patients only, 43% of university/medical school practices utilized unit-based assignments versus 48% for hospital-employed HMGs and only 32% for HMGs employed by multistate management companies. In HMGs that served pediatric patients only, 27% utilized unit-based assignments.
Undoubtedly geographic rounding has its own challenges. The pros and cons and the feasibility needs to be determined by each HMG. It’s often best to conduct the unit-based rounds on a few units and then roll it out to all the floors.
An important prerequisite to establishing a unit-based model for rounding is a detailed data analysis of total number of patients in various units to ensure there is adequate staffing. It must be practical to localize providers to different units, and complexity of various units can differ. At Lahey Hospital and Medical Center in Burlington, Mass., an efficient unit-based model has been achieved with complex units typically assigned two providers. Units including oncology and the progressive care unit can be a challenge, because of higher intensity and patient turnover.
Each unit is tagged to another unit in the same geographical area; these units are designated “sister pods.” The intention of these units is to strike a balance and level off patient load when needed. This process helps with standardization of the work between the providers. A big challenge of the unit-based model is to understand that it’s not always feasible to maintain consistency in patient assignments. Some patients can get transferred to a different unit due to limited telemetry and specialty units. At Lahey the provider manages their own patient as “patient drift” happens, in an attempt to maintain continuity of care.
The ultimate goal of unit-based assignments is to improve quality, financial, and operational metrics for the organization and take a deeper dive into provider and staff satisfaction. The simplest benefit for a hospitalist is to reduce travel time while rounding.
Education and teaching opportunities during the daily MDRs are still debatable. Another big step in this area may be a “resident-centered MDR” with the dual goals of improving both quality of care and resident education by focusing on evidence-based medicine.
Dr. Puri is a hospitalist at Lahey Hospital and Medical Center in Burlington, Mass.


