Celebrating National Hospitalist Day 2024
Many of us spend more time at work than at home, making it easy to become consumed by our jobs. When we describe ourselves, we often mention our profession first. However, we know there’s much more to life than just our work. That’s why this year’s theme for National Hospitalist Day is “Recognizing the Human in You”. It’s about acknowledging what brings us joy and sparks our interest outside of work. Some SHM members shared their stories on social media, and we are happy to share them with you. Enjoy learning more about the personal side of your fellow members.

Dr. Wray loves exploring new places on his bike.

Dr. Wray
Charlie Wray, DO, MS, is a hospitalist and assistant clinical professor of medicine at the University of California, San Francisco.
I started biking as a kid and have always loved the sport. There’s no better way to explore a new place than on a bicycle. It’s even better when you do it with friends.

Dr. Airan-Javia escapes through the creativity of pottery.

Dr. Airan-Javia
Subha Airan-Javia, MD, FAMIA, is a hospitalist and associate professor of medicine at Penn Medicine, in Philadelphia.
I believe the best kind of work is that which excites you to wake up every morning. For the past 20 years, I’ve been fortunate to experience this, serving patients as a hospitalist, enhancing the practice of medicine as a clinical informatician, innovating as a start-up CEO of CareAlign, and now making a meaningful impact through Catherine Gives, a non-profit I founded in memory of my sister Catherine who struggled with mental illness for decades. Her journey deeply influences my mission to support individuals in need.
I also believe in work hard, play hard. Alongside my professional pursuits, I treasure moments spent gardening with my daughter, gaming with my son, and creating—whether it’s through knitting, photography, or ceramic arts. These are all essential to allowing me time to unwind, create, and give to others, while still being productive!

Dr. Massart showers her teammates with baked goodies.

Dr. Massart
Annie Massart, MD, SFHM, is an assistant professor of medicine at Emory University, in Atlanta.
As an attending, I bake double batches of everything, so I’ve got plenty of snacks for my learners and the staff on the unit. Carbs are my love language, and snacks are one way that I love on all my teammates.

Dr. Thomas revels in sharing his music with the crowd.

Dr. Thomas
Joseph S. Thomas, MD, is a hospitalist at Buffalo Medical Group and a clinical instructor for the Buffalo Catholic Health System internal medicine residency and the D’Youville Physician Assistant Program, in Buffalo, N.Y. He also writes the blog Managing Health Expectations, serves as a Digital Media Fellow for the Journal of Hospital Medicine, and uses social media for education and advocacy.
When I was five years old, I wanted to do everything my father did, so I found joy in medicine and drum lessons. Drumming (both solo and in my band, Mayday Buffalo) has become my favorite release, and there are few feelings as great as a crowd of people dancing and singing along to the music I’m making!
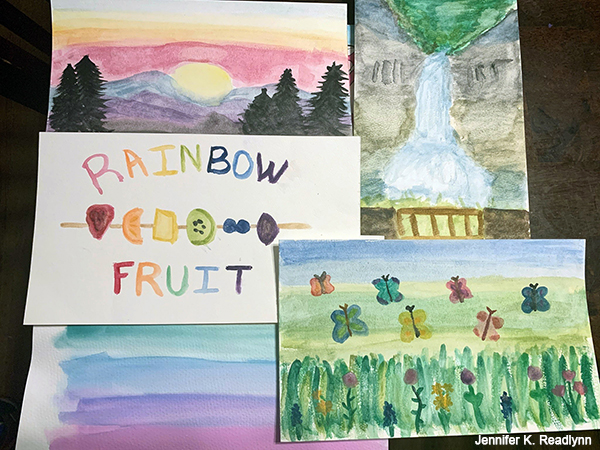
Dr. Readlynn paints watercolors with her kids.

Dr. Readlynn
Jennifer K. Readlynn, MD, FHM, is an adult hospitalist and clinician educator at the University of Rochester School of Medicine & Dentistry, in Rochester, N.Y.
I started watercolor painting during the first year of the COVID-19 pandemic. My mental health was not in a good place, and I needed something to distract me. It was also something my kids could do with me and was calming for all of us. I’m no artist but I enjoy the process regardless of the outcome and that’s a helpful mindset to get in on tough days.

Dr. Tagaram
Sandhya Tagaram, MD, FAAFP, FHM, is a hospitalist at UMass Memorial Medical Center, in Worcester, Mass.

Dr. Tagaram practices self-care through Taekwondo lessons and playing the veena.
As a physician and mom, I strongly feel that self-care is important for our emotional well-being. I enrolled in Taekwondo and South Indian music lessons along with my daughters in 2021. The tenets of Taekwondo and my journey in music have inspired me to be more mindful of the present moment and trust the process. These activities also helped me understand the concepts of self-awareness, social awareness, and the importance of lifelong learning. They have helped me to prioritize, focus, and balance my passion and goals on both personal and professional aspects. Self-care is certainly one of the virtues that I will share with my medical students, residents, and kids, which will encourage them to develop mental endurance and a resilient mind.

Dr. D’Mello relaxes by playing his guitar after a long day.

Dr. D’Mello
Kevin D’Mello, MD, FACP, FHM, is a hospitalist and associate program director, internal medicine residency at Cooper University Health Care, and associate professor of clinical medicine at Cooper Medical School of Rowan University, in Camden, N.J.
Over the past 30 years, my relationship with playing guitar has fluctuated and evolved, and today, it is a major form of relaxation for me, especially after a tough day on the floors. It perfectly combines emotion, intellect, and dexterity, and I do not need to rely on others to do it. It can purely be an expression of me.

Dr. Mandal runs the trails in the Sierra Nevada mountains.

Dr. Mandal
Atashi Mandal, MD, is a med-peds hospitalist in Southern California, whose practice encompasses both community and rural settings.
My work as a rural hospitalist introduced me to my beloved Sierra Nevada mountains. They’ve changed my life in so many good ways, and I hope to run their trails for as long as my joints will allow. The mountains appear immovable but in fact are always changing, adapting, and evolving, and I strive to follow their example with courage and compassion.

Dr. Rafiq finds pockets of meaning and inspiration among his colleagues and fellow SHM members.

Dr. Rafiq
Ali Rafiq, MD FACP, is a hospitalist with Sound Physicians at Ascension Via Christi St. Francis, in Wichita, Kan.
In a rapidly evolving world of health care, hospitalists continue to offer unique insights, thanks to our adaptability. Being a member of SHM is one of the best ways to explore this adaptability. The vision of SHM—to be the professional home of hospitalists dedicated to exceptional and equitable care for acutely ill patients—endorses our role far beyond the walls of the hospital. Handling complex tasks comes naturally to hospitalists, as we can typically maneuver through caring for sick ICU patients, attend cerebral meetings, develop organizational plans, and provide efficient care coordination, all in a day’s work.
This intensity, however, can often be paralleled with moral injury. When giving 100% to our jobs, a hospitalist’s own well-being can take a back seat. SHM offers several resources for members to counter this moral injury, and develop habits that can ensure sustainable, meaningful careers. Since the specialty is relatively new, long-term data on hospitalist well-being might be lacking. However, since we spend a humongous proportion of our lives at our workplace, it’s worthwhile to explore little pockets of meaning within the work we do. These pockets can come from enriching patient interactions, sharing a laugh with a colleague, enjoying a nutritious meal from the cafeteria, or admiring pieces of history displayed on the walls of our hospitals.
On this National Hospitalist Day, let’s work toward finding little pockets of meaning at our workplace. Let’s strive to grow and adapt together in the changing health care landscape. Let’s continue to support each other through the challenges we face, and embrace the innovation approaching us on the horizon, with the promise of delivering improved patient care. Happy National Hospitalist Day!