Though diuretics may reduce an already compromised placental blood flow by reducing intravascular volume, a number of randomized trials using diuretics have been reported. The population studied in these trials totaled approximately 7,000 individuals, and the results show no demonstrable adverse effects.5 Centrally acting alpha 2 adrenergic agonists (alpha-methyl-DOPA, clonidine), long-acting dihydropyridines (calcium channel blockers), and beta-adrenergic blockers with or without alpha-adrenergic blockade have been used successfully during pregnancy.6 Infants born to mothers receiving beta-blockers have a higher incidence of transient heart block and bradycardia. Newer agents, as opposed to alpha-methyl-DOPA and hydralazine, have not been shown to be more effective in controlling blood pressure but have demonstrated fewer adverse effects or events.
2. Mild preeclampsia may be treated using late-term delivery or bed rest before the pregnancy reaches 36 weeks. Close observation in a hospital is warranted until lack of progression to severe eclampsia is ensured.
3. Severe preeclampsia must be treated using either delivery or interventions to control blood pressure and prevent seizures while delivery is temporarily delayed to allow for fetal maturation. Intravenous magnesium sulfate (Mg2SO4), titrated to therapeutic concentrations of magnesium (4.5-8.5 mg/dl) along with suppression of deep tendon reflexes, has significantly lowered blood pressure and reduced the incidence of seizure activity. In direct comparison with intravenous phenytoin, there were no episodes of eclampsia in patients treated with magnesium (zero of 1,049 patients treated), while 10 of 1,089 individuals treated with phenytoin developed eclampsia.7 Similarly, Mg2SO4 decreased the incidence of eclampsia to 0.8% compared with 2.6% of individuals treated with nimodipine.8 Likewise, Mg2SO4 significantly reduced recurrent seizures compared to diazepam and phenytoin. In patients with renal insufficiency or other relative contraindications to Mg2SO4 therapy, the physician may treat the blood pressure with labetalol or a calcium channel antagonist and provide prophylaxis from seizures using phenytoin.
Because of the lack of a more complete understanding of the etiology (or etiologies) of preeclampsia/eclampsia, we are not fully able to identify individuals who are at risk. With further investigation, we will be able to provide more selective and effective interventions.
click for large version
click for large version
Nitrous Oxide’s Vital Role in Pregnancy
In this regard, considerable investigation has been directed toward a better understanding of eclampsia/preeclampsia in the past 20 years. The current discussion will highlight three promising lines of inquiry. Before commenting on these three areas of investigation, we feel it is important to illustrate the fundamental defect observed in all models of preeclampsia. This unifying abnormality is the presence of a placenta with inadequate uterine blood flow.
In a normal pregnancy, after implantation in the uterine wall, cytotrophoblasts invade the uterine wall, undergo a transformation of cell adhesion molecules from epithelial to endothelial expression characteristics, and induce the deep invasion of the placenta by the spiral arteries, creating large vascular sinuses in the decidua (pseudovasculogenesis). Finally, beta human chorionic gonadotropin production by the placenta stimulates the release of relaxin from the corpus luteum. Many cytokines and growth factors contribute to this normal placental development, but vascular endothelial growth factor (VEGF) and placental growth factor (PlGF) appear to be the most important.
VEGF and PlGF play an integral role in the inducement of conversion of the cytotrophoblast cell adhesion molecules from epithelial to endothelial expression, particularly integrins and cadherins. In models of preeclampsia, there is insufficient invasion of the spiral arteries and inadequate uterine blood flow, as well as a lack of alteration in adhesion molecules of cytotrophoblasts and failed pseudovasculogenesis.9
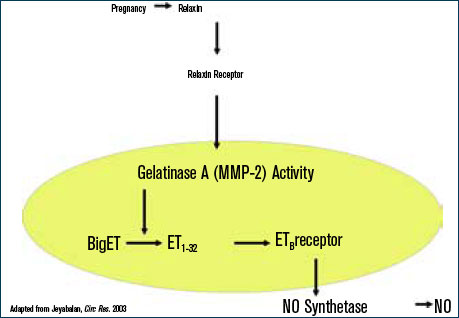
During normal pregnancy, intravascular volume increases, peripheral vascular resistance (PVR) decreases, and renal blood flow and glomerular filtration rate (GFR) increase. (See Figure 1, above left.) Concomitant with the increased plasma volume, the reduction of PVR (vasodilation) not only mitigates the effect of plasma volume on systemic blood pressure, but actually reduces the systemic blood pressure during normal pregnancy. (See Figure 2, below.) Based on seminal studies by Jeyabalan and colleagues, one explanation for the decline in PVR and blood pressure, along with the increased renal plasma flow and GFR, is the production and action of relaxin on vascular smooth muscle to stimulate gelatinase-A (matrix metalloproteinase-2), which cleaves bigET (endothelin precursor) to form ET1-32. (See Figure 3, above.) ET1-32 binds to the ETB receptor and increases nitrous oxide (NO) synthetase activity and NO production, leading to vasodilation.10