A75-year-old previously healthy woman presented with one-month history of extensive necrotic coalescing erythematous weeping vesicles and bullae. A skin biopsy was performed. (See right and right bottom for images.)
Based on the skin biopsy and clinical presentation, the most likely diagnosis is:
- Pemphigoid;
- Pemphigus vulgaris;
- Staphylococcus scalded skin syndrome;
- Porphyria cutanea tarda; or
- Darier’s disease.
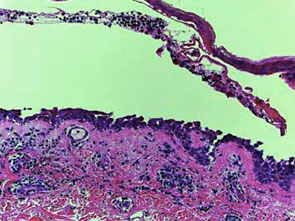
The results of the patient’s skin biopsy.

The patient presented with extensive necrotic coalescing erythematous weeping vesicles and bullae.
Discussion
The correct answer is B: pemphigus vulgaris. The skin biopsy demonstrates an intra-epidermal split along the basal layer of keratinocytes. The basal cells along the basement membrane zone demonstrate tombstoning consistent with pemphigus vulgaris. Clinically, she has erythematous superficial erosions with slight re-epithelialization.
Pemphigoid is another blistering disorder that often affects the elderly and classically presents with tense bulla that demonstrate an infra-basilar split on histology. Staphylococcus scalded skin syndrome may present similarly, but histology shows acantholysis in the superficial epidermis. Porphyria cutanea tarda often is on the hands, arms, and other sun-exposed areas, and biopsy reveals dermal papillae protruding up toward the bulla (festooning). Darier’s disease is autosomal dominant and presents with greasy hyperkeratotic papules that show acantholysis and dyskeratosis on histology, with occasional suprabasal clefting.
Pemphigus vulgaris is an autoimmune process that often affects those in middle age. It usually first involves the mucous membranes and then progresses to the skin, where intraepidermal bullae form. These bullae are flaccid and easily rupture, often easily extending beyond their original dimensions with only slight perturbation. Because of their fragility patients may not present with any intact bullae and instead only have painful erosions, as in this case.
The disease is mediated by circulating immunoglobulin G (IgG), which binds to the cell surface of keratinocytes, breaking up intercellular connections and resulting in acantholysis and bulla formation. The process is diagnosed with the shown histology and with direct in vivo immunofluorescence, which demonstrates a “chicken-wire” pattern around keratinocytes. Paraneoplastic pemphigus and pemphigus foliaceous are the other two types of pemphigus, and a work up for underlying malignancy is indicated to rule out the former. Opportunistic infections are common and can lead to exacerbation of the disease, so culture and antimicrobial therapy often play an important role in recovery.
Pemphigus can often be controlled with adequate immunosuppression. High-dose systemic steroids are the first-line treatment. Other immunosuppressive medications, such as dapsone, azathioprine, and mycophenolate mofetil, are used for maintenance therapy during and after the patient has recovered from a flare-up. Intravenous immunoglobulin (IVIG) and plasmapheresis therapy has also showed promising results.1,2
This case was complicated by superinfection with both methicillin-resistant staphylococcus aureus (MRSA) and herpes simplex virus. One course of IVIG produced no benefit. The patient then underwent intensive inpatient wet-dressing therapy with topical steroids and antimicrobial treatment. She was placed on high-dose prednisone and began to recover, without new lesion development and with re-epithelialization. First mycophenolate mofetil followed by azathioprine were started, to which the patient responded well. TH
References
- Bystryn JC, Rudolph JL. IVIG treatment of pemphigus: how it works and how to use it. J Investig Dermatol. 2005 Dec;125(6):1093-1098.
- Stanley JR. Therapy of pemphigus vulgaris. Arch Dermatol. 1999 Jan;135(1):76-78.